

Bladder Cancer
Understanding Staging and Grading
Determining the type of bladder cancer you have and its extent will be the first goal of your physician. Once a diagnosis is made, your doctor will classify and stage the cancer according to the TNM system developed by the American Joint Committee on Cancer (AJCC).
This system classifies the cancer by tumor (T), node (N) and metastasis (M). The T category describes the size and location of the primary tumor. The N category indicates whether the lymph nodes show evidence of cancer cells. The number and location of these lymph nodes are important because they show how far the disease has spread. The M category describes metastasis (spread of cancer to another part of the body), if any. Once the cancer is classified, an overall stage is assigned (see Tables 1 and 2).
Another important characteristic of the cell in a urothelial cancer is the grade (G); grade is determined by how much the cancer cells look like healthy cells when viewed under a microscope (see Table 3, page 2). The grade is an imprecise indication of how likely the cancer is to recur, grow or spread. If cancer has spread beyond the bladder, your doctor may recommend genomic testing, which may influence treatment.
The Role of Genomic Testing
Genomic testing is used to examine a cancer’s genes to identify mutations that could indicate the cancer’s behavior, how aggressive it might be and whether it will metastasize (spread). This information can lead to a more precise diagnosis and a more personalized treatment plan. Genomic testing is performed on a sample of tumor tissue, which is typically taken during the diagnostic process
Genomic testing is increasingly being used to determine whether bladder cancer has certain gene variants, which may code for substances that may provide a target that could be “attacked” by a specific drug. If a mutation is found, your doctor will select a drug therapy that may target that specific mutation. However, not all mutations or variants provide substances for which there is a specific and approved treatment available.
Research has uncovered multiple gene mutations that contribute to bladder cancer, and additional mutations are expected to be found in the future. Some of the common gene mutations found in bladder cancer include the following: ATM/RB1, ERCC2, FGFR2, FGFR3, HER2, HRAS, PIK3CA, TP53 and TSC1. If the testing does not identify a “targetable abnormality” for which a specific treatment is available, there are still several very effective approaches available; these may entail standard of care or clinical trials as options to consider.
In rare cases, bladder cancer can be inherited. But your doctor may recommend genetic testing if you have a family history of bladder cancer.
Illustrated Stages of Bladder Cancer
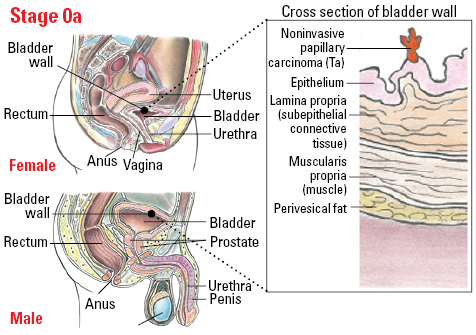

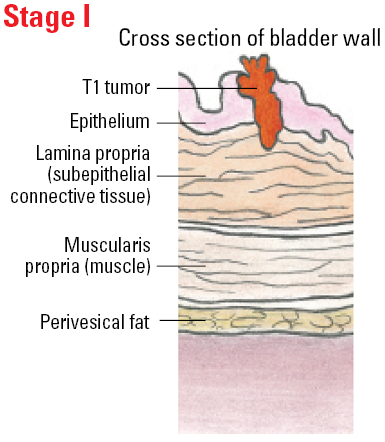
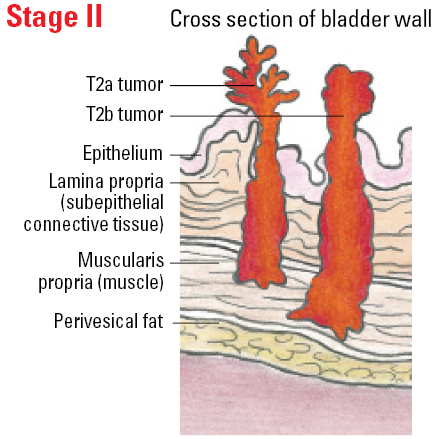
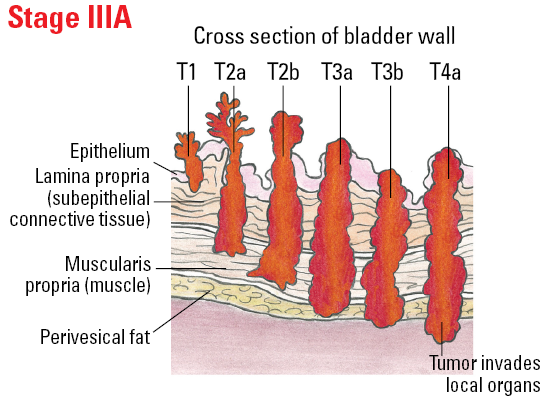
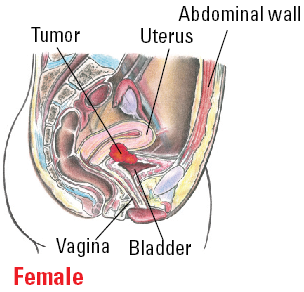


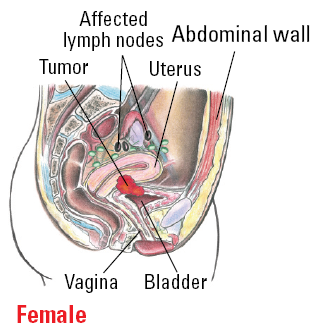

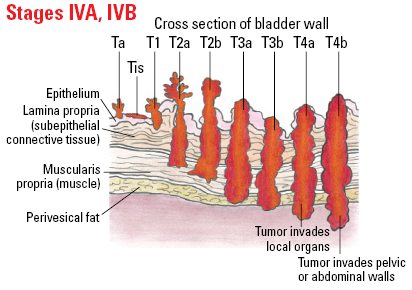
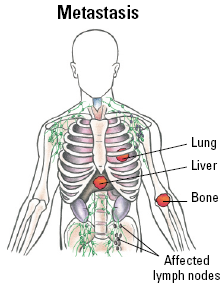
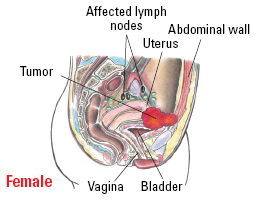
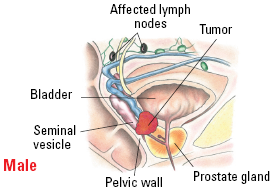
Table 1. AJCC System for Bladder Cancer
| Category | Definition | |
| Tumor (T) | ||
| TX | Primary tumor cannot be assessed | |
| T0 | There is no evidence of primary tumor | |
| Ta | A papillary carcinoma is detected but is considered to be noninvasive | |
| Tis | There is evidence of a noninvasive flat carcinoma (flat carcinoma in situ, or CIS) | |
| T1 | The tumor has grown from the inner lining of the bladder to the connective tissue, but hasn't yet spread to the muscle layer of the bladder | |
| T2 | The tumor has invaded the muscle layer of the bladder | |
| T2a | The tumor has grown into only the inner half of the muscle layer | |
| T2b | The tumor has grown into the outer half of the muscle layer | |
| T3 | The tumor has grown through the muscle into the fatty tissue (also known as the perivesicle fat or serosa) | |
| T3a | Invasion of the tumor to the serosa can be seen only through a microscope | |
| T3b | Invasion of the tumor to the serosa can be felt by the surgeon or seen on imaging tests | |
| T4 | The tumor has spread beyond the bladder and may be growing into surrounding organs, seminal vesicles and the pelvic and abdominal wall | |
| T4a | The tumor has spread to the prostate in me or to the uterus and/or vagina in women | |
| T4b | The tumor has spread to the pelvic wall or abdominal wall | |
| Nodes (N) | ||
| NX | Regional lymph nodes cannot be assessed | |
| N0 | Cancer has not spread to regional lymph nodes | |
| N1 | Cancer has spread to one pelvic lymph node | |
| N2 | Cancer has spread to two or more pelvic lymph nodes | |
| N3 | Cancer has spread to lymph nodes along the common iliac artery | |
| Metastasis (M) | ||
| M0 | Cancer has not spread to distant areas of the body | |
| M1 | Cancer has spread to distant areas of the body (most commonly to distant lymph nodes, bones, the lungs and/or the liver) | |
Table 2. Stages of Bladder Cancer
| Stage | TNM Classifications | ||
| 0a | Ta | N0 | M0 |
| 0is | Tis | N0 |
M0
|
| I | T1 | N0 | M0 |
| II | T2a or T2b | N0 | M0 |
| III | T3a, T3b or T4a | N0 | M0 |
| IV |
Tb4
Any T Any T |
N0
N1, N2 or N3 Any N |
M0
M0 M1 |
Table 3. Grades of Bladder Cancer
| Classification | Definition | ||
| Urothelial Histologies | |||
| LG | Low-grade. | ||
| HG | High-grade. | ||
| Squamous Cell Carcinoma and Adenocarcinoma | |||
| GX | Grade cannot be assessed. | ||
| G1 | Well differentiated. | ||
| G2 | Moderately differentiated. | ||
| G3 | Poorly differentiated. | ||
