Head & Neck
Major Salivary Gland Cancer
Includes illustrated staging details
Your head and neck contain salivary glands that help you lubricate, swallow and digest food and keep your mouth and throat moist. The enzymes within saliva begin the process of breaking down food while antibodies help prevent infections in the mouth and throat.
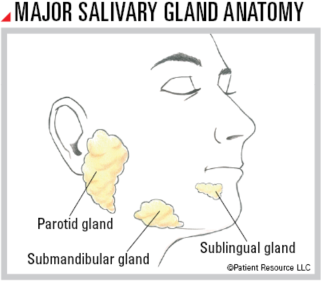
You have major and minor salivary glands, with a set of three major glands on each side of your face:
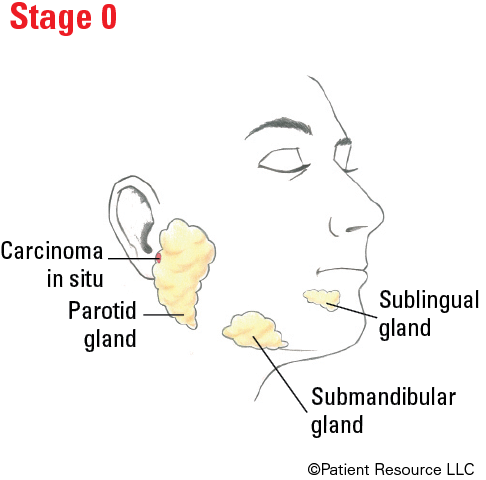
- The parotid glands are the largest of the major glands and are located just in front of each ear.
- The submandibular glands below your mandible (jawbone) are smaller.
- The sublingual glands under the mouth floor are the smallest.
You also have hundreds of minor salivary glands.
Tumors most often occur in the parotid glands. Tumors in the minor salivary glands are not common; however, they are more likely to be malignant when they occur.
Treatment Options
When developing your treatment plan, your doctor will consider the subtype, stage and grade of your cancer. Multiple subtypes have been identified in major salivary gland cancer. In general, the lower the tumor grade, the better the prognosis (outlook). Your overall health, the impact to your speech, chewing and swallowing, and your preferences are also considered.
Talk with your doctor about the benefits and risks as well as the potential side effects and late effects of each type of therapy before making decisions.
One or more of the following options may be part of your treatment plan.
Surgery is the most common treatment for major salivary gland cancer to remove the tumor and surrounding tissue. More than one surgery may be needed to treat the cancer and to repair the area (see Reconstruction & Rehabilitation). One of the following procedures may be used.
Superficial parotidectomy may be used to remove cancer in the outside part of the parotid gland, also known as the superficial lobe. This involves removing the lobe.
Total parotidectomy to remove the entire parotid gland may be used if the cancer extends to deeper tissues. Removal of the facial nerve may be required, which would affect facial movement.
A neck dissection to remove some lymph nodes in your neck may be recommended. Your doctor will consider the exact location and stage of your tumor.
Other surgical procedures are available depending on the diagnosis.
Radiation therapy may be recommended for intermediate or high grade or advanced salivary gland cancers after surgery (adjuvant therapy) to kill remaining cancer cells. If surgery is not an option, radiation may be the main treatment, but radiation therapy may not be effective alone against some salivary gland tumors. It is sometimes used to manage symptoms of pain, bleeding or trouble swallowing and in cases of recurrent or advanced salivary gland cancer. Two main types of radiation may be used.
External-beam radiation therapy (EBRT) uses a machine outside the body to send radiation toward the cancer. Different types of EBRT are available and include intensity-modulated radiation therapy; proton therapy, which uses charged particles called protons; and fast neutron radiation therapy, which uses neutrons.
This treatment may also be combined with chemotherapy, known as chemoradiation.
Drug therapy may be recommended for some cases. It is typically reserved for patients with late-stage cancer or to relieve symptoms.
Chemotherapy is the main type of drug therapy chosen to treat salivary gland cancer.
Immunotherapy in the form of immune checkpoint inhibitors may be used to treat recurrent or metastatic salivary gland cancer that has stopped responding to chemotherapy. The doctor will test for the tumor’s PD-L1 expression, which may indicate whether the tumor could respond to immunotherapy, and for tumor mutational burden (TMB). If PD-L1 expression is more than 1 percent, the tumor is considered to be PD-L1 positive and immunotherapy alone may be used. If PD-L1 is negative, immunotherapy and traditional chemotherapy are often combined for recurrent or metastatic cancer. If TMB is high, this treatment may also be an option.
Targeted therapy may be an option for some subtypes of salivary gland cancer through clinical trials. This type of personalized treatment attacks the source of a tumor’s growth, focusing on certain parts of cells and the signals that cause them to grow unchecked or keep from dying. In salivary gland cancer, some of these drugs also target specific genes or molecular alterations, including neurotrophic tyrosine receptor kinase (NTRK), human epidermal growth factor receptor-2 (HER2) and epidermal growth factor receptor (EGFR).
TNM Classification for Major Salivary Gland Cancer
| Classification | Definition |
| Tumor (T) | |
| TX | Primary tumor cannot be assessed. |
| T0 | No evidence of primary tumor. |
| Tis | Carcinoma in situ. |
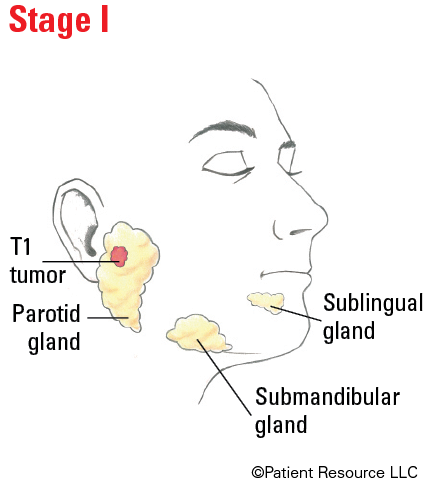
| T1 | Tumor 2 cm or smaller in greatest dimension without extraparenchymal extension (spread to surrounding tissues). |
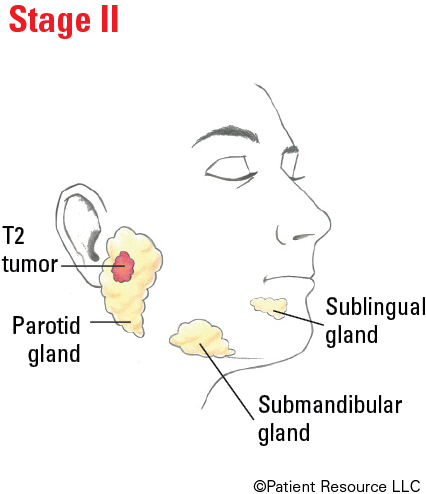
| T2 | Tumor larger than 2 cm but not larger than 4 cm in greatest dimension without extraparenchymal extension (spread to surrounding tissues). |
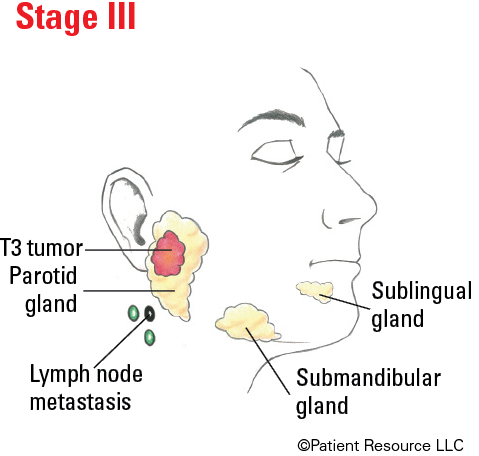
| T3 | Tumor larger than 4 cm and/or tumor having extraparenchymal extension (spread to surrounding tissues). |
| T4 | Moderately advanced or very advanced disease. |
| T4a |
Moderately advanced disease.
Tumor invades skin, mandible (lower jaw), ear canal, and/or facial nerve. |
| T4b |
Very advanced local disease.
Tumor invades skull base and/or pterygoid plates and/or encases carotid artery. |
| Node (N) | |
| NX | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis. |
| N1 | Metastasis in a single ipsilateral (on the same side) lymph node, 3 cm or smaller in greatest dimension and ENE*(-). |
| N2 |
Metastasis in a single ipsilateral (on the same side) lymph node, 3 cm or smaller in greatest dimension and ENE*(+);
or larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(-); or metastases in multiple ipsilateral lymph nodes, none larger than 6 cm in greatest dimension and ENE(-); or in bilateral (on both sides) or contralateral (on the opposite side) lymph node(s), none larger than 6 cm in greatest dimension, ENE(-). |
| N2a |
Metastasis in single ipsilateral (on the same side) node 3 cm or smaller in greatest dimension and ENE*(+);
or a single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(-). |
| N2b | Metastases in multiple ipsilateral (on the same side) nodes, none larger than 6 cm in greatest dimension and ENE*(-). |
| N2c | Metastases in bilateral (on both sides) or contralateral (on the opposite side) lymph node(s), none larger than 6 cm in greatest dimension and ENE*(-). |
| N3 |
Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE*(-);
or metastasis in a single ipsilateral (on the same side) node larger than 3 cm in greatest dimension and ENE(+); or multiple ipsilateral, contralateral (on the opposite side) or bilateral (on both sides) nodes, any with ENE(+); or a single contralateral node of any size and ENE(+). |
| N3a | Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE(-). |
| N3b |
Metastasis in a single ipsilateral (on the same side) node larger than 3 cm in greatest dimension and ENE*(+);
or multiple ipsilateral, contralateral (on the opposite side) or bilateral (on both sides) nodes, any with ENE(+); or a single contralateral node of any size and ENE(+). |
| Metastasis (M) | |
| M0 | No distant metastasis. |
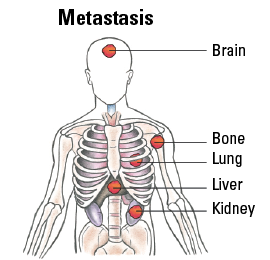
| M1 | Distant metastasis. |
Staging Major Salivary Gland Cancer
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III |
T3 T0, T1, T2, T3 |
N0 N1 |
M0 M0 |
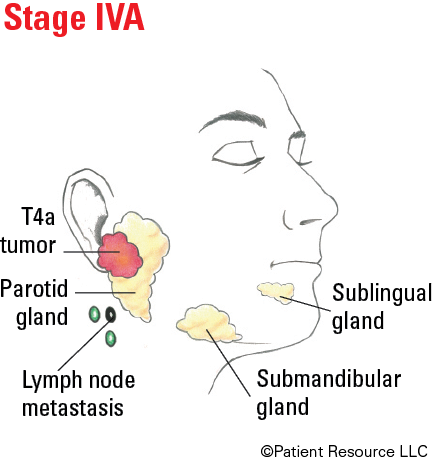
| IVA |
T4a T0, T1, T2, T3, T4a |
N0, N1 N2 |
M0 M0 |
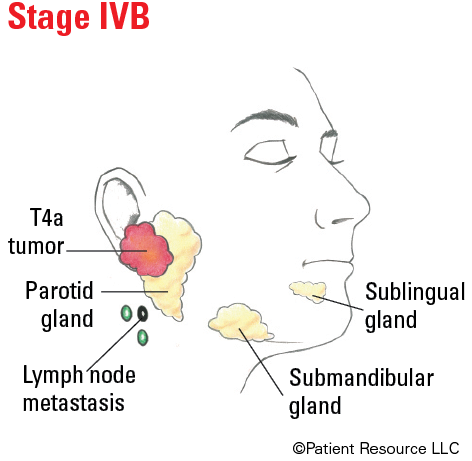
| IVB |
Any T T4b |
N3 Any N |
M0 M0 |
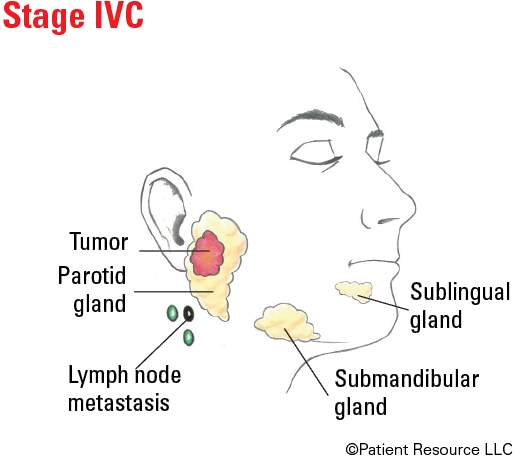
| IVC | Any T | Any N | M1 |
Illustrated Stages of Major Salivary Gland Cancer