
Lung Cancer
Treatment Planning
Approaches for treating and managing lung cancer diagnoses have improved a great deal recently, and especially in the past five years. New drug therapies, biomarker testing and early detection are revolutionizing how doctors find and treat non-small cell lung cancer (NCLC) and small cell lung cancer (SCLC). As a result, more people are living longer with lung cancer. Even better, research shows no signs of slowing down any time soon, offering hope for a cure.
Because so many advances continue to happen, the NSCLC landscape is constantly changing. To have access to the latest treatments, you are encouraged to find a health care provider who specializes in lung cancer to help you understand all of the options.
Your treatment plan will be based on the results of your diagnostic testing, staging and the presence of biomarkers. Everyone with NSCLC, except for those with Stage I diagnoses, should have biomarker testing because drug therapy will likely be used in addition to surgery or radiation therapy for early stages (II and III) and alone for Stage IV. Drug treatment will be done either before (neoadjuvant) and/or after (adjuvant) surgery for early stages and generally after radiation therapy of Stage III. Knowing the biomarkers you have can help your health care provider create a more personalized treatment plan for your specific cancer.
Types of Treatment
Your treatment plan may include one or more of the following.
Surgery
This is typically the primary treatment for early-stage (Stages I, II and some IIIA) NSCLC tumors. It is not commonly used for SCLC and is typically reserved only for very early-stage SCLC disease (Stage I), which is uncommon. In this case, chemotherapy is administered after surgery. In some cases when cancer has spread to the brain, surgery may be used.
If you are a candidate for surgery, a board-certified thoracic surgeon who is experienced in lung cancer should determine whether the tumor(s) can be successfully removed. The procedure selected will depend on how much of your lung is affected, tumor size and location and your overall health.
The following types of surgery may be done by open thoracotomy (a large incision in the chest wall that requires separation of the ribs) or by less invasive procedures, such as video-assisted thoracoscopic surgery (VATS) with or without robotic surgery.
Open surgery options include:
- Wedge resection to remove the tumor with a triangular piece of a lobe of the lung.
- Segmental resection (segmentectomy) to remove a larger section of a lobe.
- Lobectomy to remove one of the lungs’ five lobes.
- Pneumonectomy to remove an entire lung.
- Sleeve resection (sleeve lobectomy) to remove part of the bronchus (main airway) or pulmonary artery to the lung along with one lobe to save other portions of the lung.
VATS is performed as the surgeon inserts scopes through small incisions. These procedures may help preserve muscles and nerves, reduce complications and shorten recovery time. Robotic surgery may be used to remove some early-stage tumors. Special equipment provides a three-dimensional view inside the body while the surgeon guides a robotic arm and high-precision tools that can bend and rotate much more than the human wrist. Neurosurgery may be an option for treating brain metastases. Finding a surgeon with extensive training and experience is highly recommended.
Drug Therapy
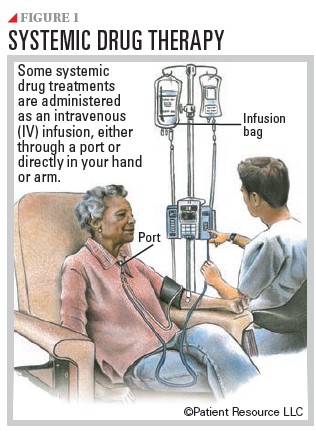
Drug therapies may be used alone or in combination. Some are systemic, meaning they travel throughout the body.
Chemotherapy may be a part of the treatment plan for some stages of NSCLC and is the primary treatment for all stages of SCLC. Chemotherapy is a drug that kills rapidly dividing cells, which includes cancer cells but also some healthy cells like those in the bone marrow, digestive tract and hair follicles. It may be given alone or in combination with surgery, radiation therapy or immunotherapy.
In early-stage NSCLC, it may be used before surgery to help shrink the tumor, after surgery to kill remaining cells, as maintenance therapy following standard chemotherapy to prevent recurrence, or as palliative care to help relieve symptoms.
For some Stage III diagnoses, a combination of chemotherapy and radiation therapy may be used and followed by immunotherapy.
For metastatic NSCLC, chemotherapy may be combined with immunotherapy (chemoimmunotherapy) or targeted therapy. Most often platinum-doublet chemotherapy may be used. This treatment regimen combines a platinum-based chemotherapy with a second chemotherapy drug, forming a “doublet.” It is a standard first-line treatment for advanced NSCLC.
For limited-stage SCLC, chemotherapy is often combined with radiation therapy to the chest (chemoradiation) followed by immunotherapy. In extensive-stage SCLC, chemotherapy is combined with immunotherapy (chemoimmunotherapy). Chemotherapy is also used for second-line treatment for SCLC. If there is a recurrence, depending on how quickly the cancer returned, the first chemotherapy combination may be used again in the second-line setting if there was a good and long-lasting response to therapy. If there was not, other chemotherapy drugs are approved to treat SCLC as second-line therapy, or a different combination of chemotherapy drugs may be used.
Immunotherapy helps the body’s immune system recognize and destroy cancer cells. By training the immune system to respond to cancer, this strategy has the potential for a response that can extend beyond the end of treatment. It may be used alone or in combination with other types of immunotherapy or chemotherapy. Most immunotherapies are intravenously administered antibodies that target proteins that prevent the immune system from killing the cancer.
Immunotherapy alone or combined with chemotherapy is standard first-line therapy for Stage IV NSCLC without specific genetic mutations and is approved in combination with platinum-doublet chemotherapy (chemoimmunotherapy) as neoadjuvant therapy for early-stage NSCLC. It is standard after chemotherapy and radiotherapy for inoperable (unresectable) Stage III NSCLC. If you cannot have platinum-doublet chemotherapy, you may be given double immunotherapy, which includes two types of immunotherapy. Immunotherapy after chemoradiation is standard in limited-stage SCLC. Immunotherapies combined with chemotherapy is standard for extensive-stage SCLC. A new type of immunotherapy known as a bispecific T-cell engager was recently approved for extensive-stage SCLC with disease progression on or after platinum-based chemotherapy.
The types of immunotherapy approved to treat lung cancer include the following.
Immune checkpoint inhibitors prevent the immune system from slowing down and help the immune system keep up its fight against cancer. Three types of checkpoints can be treated with immunotherapy. The most common you will hear about is PD-L1 (programmed death-ligand 1). Depending on your diagnosis, your doctor may test for the tumor’s PD-L1 expression. Tumors that have a high level of PD-L1 are considered good candidates for treatment with immunotherapy because they tend to respond well.
Bispecific T-cell engagers (BiTEs) fight SCLC in two different ways. BiTEs connect a T-cell, which is a type of white blood cell that is part of the immune system, with a tumor cell. When a BiTE connects a T-cell directly to a tumor cell, it releases chemicals or other therapeutics to attack the tumor from inside the cell. Normally, a T-cell can only interact with a tumor cell if it finds an antigen on a tumor cell and connects to it. Antigens are any substances that cause the body to make an immune response against that substance.
Chemoimmunotherapy combines chemotherapy with immunotherapy. It may be used to treat early-stage NSCLC before or after surgery or both. It may be used in Stage IV NSCLC if there are no biomarkers and if the PD-L1 score is less than 50. This therapy is currently the preferred first-line treatment option for the majority of advanced NSCLC diagnoses without biomarkers and is the preferred treatment for extensive-stage SCLC.
Targeted therapy may treat tumors with or without driver mutations, which are changes in genes that cause cells to become cancer cells that grow and spread in the body. They “drive” the development of cancer.
Most targeted therapies are given orally as a pill and are recommended as first-line therapy for NSCLC. If the drug used in the first-line therapy is not effective, another one may be considered. To determine whether you are a candidate for targeted therapy, a biopsy tissue sample and blood sample must be tested at a specialized lab to detect any known biomarkers. This should be done before your treatment begins. Ask your doctor whether tissue from a previous biopsy can be used, if applicable. The driver mutations that have targeted therapies approved to treat them include:
- ALK fusions
- BRAF V600E mutations
- EGFR mutations
- HER2 (ERBB2) mutations
- KRAS mutations
- MET exon 14 skipping mutations
- NRG1 fusions
- NTRK fusions
- RET fusions
- ROS1 fusions
If your tumor does not have a biomarker or has tested positive for a biomarker that does not have an approved targeted treatment, ask your doctor about participating in a clinical trial. You may be eligible.
Types of targeted therapy approved for NSCLC include tyrosine kinase inhibitors (TKIs), monoclonal antibodies (mAbs), angiogenesis inhibitors and antibody drug conjugates (ADC).
Tyrosine kinase inhibitors (TKIs) block enzymes responsible for certain functions within a cell. These enzymes may be too active or found at high levels in some cancer cells. Blocking them may help keep cancer cells from growing.
Monoclonal antibodies (mAbs) are laboratory-made antibodies designed to target specific tumor antigens, which are substances that cause the body to make a specific immune response. They can work in different ways, such as flagging targeted cancer cells for destruction, blocking growth signals and receptors, and delivering other therapeutic agents directly to targeted cancer cells
Angiogenesis inhibitors shut down vascular endothelial growth factor (VEGF), a protein that is essential for creating blood vessels. Solid tumors need a blood supply if they are going to grow beyond a few millimeters. But with no vessels to supply blood, the tumor eventually “starves” and dies. Angiogenesis inhibitors are often given in combination with chemotherapy.
Antibody drug conjugates (ADCs) are a type of monoclonal antibody (mAb) that is chemically linked to a chemotherapy drug. ADCs target only cancer cells, leaving healthy cells alone. The mAb binds to specific proteins or receptors found on certain types of cells, including cancer cells. The linked chemotherapy drug enters these cells and kills them without harming other cells. An ADC has been approved to treat the human epidermal growth factor receptor-2 (HER2) mutation, also known as ERBB2. Other ADCs are being investigated in clinical trials.
Radiation therapy
Also called radiotherapy, radiation therapy uses high-energy radiation to destroy cancer cells and shrink tumors. It is often combined with other treatment types for NSCLC and SCLC. It may also be used as palliative care to help relieve pain from cancer that spreads to the bone.
External-beam radiation therapy (EBRT) is the most common form of radiation therapy used. EBRT comes in multiple forms:
- Three-dimensional conformal radiation therapy (3D-CRT) uses precise mapping to shape and aim radiation beams at the tumor(s) from multiple directions, typically causing less damage to normal tissue.
- Stereotactic body radiotherapy (SBRT) is a form of 3D-CRT offering precision delivery of high-dose radiation through beams aimed at the tumor from multiple directions. SBRT may be the primary treatment for small tumors or early-stage cancers when a person cannot undergo surgery or makes the decision not to have surgery.
- Intensity-modulated radiation therapy (IMRT) is an advanced form of 3D-CRT that delivers radiation from a machine that moves around the person, aiming beams at varying strengths for increased precision. This technique may be used to treat tumors located near sensitive areas such as the spinal cord.
- Proton beam therapy destroys cancer cells by using charged particles called protons. This treatment typically results in less damage to healthy tissue and fewer side effects than traditional radiation therapy.
- Volumetric arc-based therapy (VMAT) delivers IMRT in an arc shape around the tumor(s).
For NSCLC, radiation therapy can be used after surgery to treat any remaining cancer. It may also be combined with chemotherapy (chemoradiation), be the primary therapy for Stage I and some Stage II tumors, treat where the tumor has spread, including the brain, or alleviate bone pain from metastases.
For SCLC, radiation therapy is used for limited-stage SCLC that has not spread to the lymph nodes and cannot be treated with surgery. It is often combined with chemotherapy in a treatment called chemoradiation. People with extensive-stage SCLC may receive radiation therapy to treat remaining disease in the chest.
If a complete or partial remission is seen after first-line treatment for limited-stage SCLC, your doctor may offer prophylactic (preventive) cranial irradiation (PCI) using SBRT to prevent the spread of SCLC to the brain. Before moving forward, talk with your doctor about the potential advantages and risks of this approach for your specific situation.
Chemoradiation
Also called chemoradiotherapy or concurrent chemoradiation, this treatment combines chemotherapy with radiation therapy. It makes cancer cells more sensitive to radiation, making it easier for the radiation therapy to kill them. It is an option for some Stage IIB and Stage III NSCLCs. People with limited-stage SCLC are usually treated with chemotherapy and radiation therapy given concurrently for two of four chemotherapy cycles.
Radiofrequency ablation
This therapy may be used to treat small NSCLC tumors when surgery is not an option. A needle placed directly into the tumor passes a high-frequency electrical current to the tumor that destroys cancer cells with intense heat. It is rarely used for SCLC tumors.
Cryosurgery
Also called cryoablation and cryotherapy, cryosurgery kills cancer cells by freezing them with a probe or another instrument that is super-cooled with liquid nitrogen or similar substances. An endoscope, which is a thin tube-like instrument, is used for this procedure to treat NSCLC tumors in the airways of the lungs. It is not used to treat SCLC.
Photodynamic therapy
This treatment kills cancer cells by injecting a drug that has not yet been exposed to light into a vein. The drug is drawn to cancer cells more than normal cells. Fiber optic tubes are then used to carry a laser light to the cancer cells, where the drug becomes active and kills the cells. It is used mainly to treat tumors on or just under the skin or in the lining of internal organs. When the tumor is in the airways, therapy is directed to the tumor through an endoscope. It may help relieve breathing problems or bleeding in NSCLC and can also treat small tumors. It is not used for SCLC.
Consolidation and Maintenance Therapy
Consolidation therapy is treatment that is given after cancer has partially responded to initial therapy. It is used to kill any cancer cells that may be left in the body. It may include radiation therapy, surgery or drug therapies designed to kill cancer cells.
Maintenance therapy is treatment that is given after first-line therapy. It is given to help keep cancer from coming back after it has disappeared following therapy.
Recurrence, Resistance and Follow-up Care
Both NSCLC and SCLC can return after treatment. A recurrence happens when some tiny cancer cells remain in your body after treatment. Over time, these cells divide and grow into cancer again. It may come back in your lungs or a different part of your body, such as the brain, opposite lung, bone or liver. It can happen weeks, months or even years after treatment stops.
Catching a recurrence as soon as possible will help your doctor determine the next best treatment for you. A recurrence may be found through routine follow-up screening with scans or bloodwork. If you experience the following symptoms, you should contact your health care provider right away: A cough that doesn’t go away, chest pain, shortness of breath, lung infections, such as bronchitis and pneumonia, blood when you cough, pain, fatigue, skin issues, fever or unexplained weight loss.
Get immediate help for sudden or serious symptoms, such as high fever, severe pain or difficulty breathing.
Treatment options after first-line therapy failure will depend on how soon the recurrence happens after treatment ended as well as the cancer’s stage after the recurrence has been confirmed. Some people mistakenly believe that if the first treatment fails or stops working, they have no other options. However, recent advances in treatment now offer several second-line options for both NSCLC and SCLC. Before beginning your first treatment, it may be a good idea to talk with your health care provider about what your treatment options will be if the first therapy stops working.
Early detection may improve prognosis. Additionally, regular preventive medical appointments promote overall health and awareness of other diseases and illnesses.
Being aware that cancer may return after your initial therapy is important, as is understanding resistance. Resistance is believed to develop when some cancer cells survive after being treated. The surviving cells recover and begin to grow and divide again, often with new genetic changes that the initial treatment is not designed to target.
Research is underway to understand how and why resistance develops and to find ways to prevent it or slow it down to extend the effectiveness of the original therapy. Some people with lung cancer develop resistance to some forms of therapy, which decreases the response and success of treatment. The most well-known treatment that can develop resistance in lung cancer is targeted therapy. However, it can also happen with chemotherapy, radiotherapy and immunotherapy.
In rare cases, NSCLC cells can transform into SCLC. Known as transformed small cell lung cancer (tSCLC), it most often occurs in NSCLC that has the EGFR biomarker and usually contains both NSCLC and SCLC cells. Treatments may consist of combined therapies used to treat both NSCLC and SCLC.
As of 10/1/25
Stay on Track and On Time With All Medications
Advances in cancer treatment have made oral therapies (pills) an option for many types of cancer. If your health care provider prescribes an oral therapy, you will likely enjoy the convenience of taking a pill instead of going for treatment that may take up to several hours. Along with that convenience, however, comes the responsibility of taking the therapy in the correct way.
Taking your medication exactly as prescribed by your doctor is called medication adherence, and it is extremely important in the treatment of NSCLC. Most cancer therapies are designed to maintain a specific level of drugs in your system for a certain time based on your cancer type and stage, your overall health, previous therapies and other factors. If your oral therapies are not taken as prescribed, or if you miss appointments for your IV infusions, injections or radiation therapy, the consequences can be serious — even life threatening.
A variety of tools can help you stay on track with medications and appointments:
- Write down when you take your medications and go to appointments.
- Talk to your pharmacist to ensure you understand how to take your medications.
- Use an alarm on your phone, clock or computer as a reminder.
- Enlist a caregiver to help remind you.
Download the Patient Resource Medication Journal to keep track of your medications at PatientResource.com/Medication_Journal
Words to Know
As you learn about your lung cancer diagnosis, it is important to understand the words you may hear from your health care team. These explanations may help you feel more informed as you make the important decisions ahead.
First-line therapy is the first treatment used.
Maintenance therapy can be given after first-line therapy to help keep cancer from coming back after it has disappeared following therapy.
Second-line therapy is given when the first-line therapy does not work or is no longer effective.
Standard of care refers to the widely recommended treatments known for the type and stage of cancer you have.
Neoadjuvant therapy is given to shrink a tumor before the primary treatment (usually surgery). It may also be referred to as preoperative therapy.
Adjuvant therapy is additional cancer treatment given after the primary treatment (usually surgery or radiotherapy) to destroy remaining cancer cells and lower the risk that the cancer will come back. It may also be referred to as postoperative therapy.
Local treatments are directed to a specific organ or limited area of the body and include surgery and radiation therapy.
Systemic treatments travel throughout the body and are typically drug therapies, such as chemotherapy, molecular therapy, targeted therapy and immunotherapy.
Response to therapy means that the cancer has reduced in size or lost its blood supply in a manner that can be measured by CT or MRI.
Page Navigation
