
Liver Cancer
Treatment Planning
Much discussion will happen before your treatment plan is decided, and you will be at the heart of it. Ask questions and give your input, then keep the lines of communication open. The more you know, the better equipped you will be to manage your hepatocellular carcinoma (HCC).
Your doctor will evaluate all of these:
- The results of a thorough health assessment, diagnostic tests and imaging
- How much of your liver is affected by the tumor
- The number of tumors, including their size and location
- Whether the cancer has metastasized (spread) outside the liver
- Whether your tumor has grown into blood vessels of the liver
- How well your liver is working
- Any health areas of your liver
- Any comorbidities (other serious health conditions)
- Your overall physical condition
- Expectations for your quality of life
Next, you will talk about your goals of treatment. Your prognosis (outlook) will help guide this discussion. Your goals may change as your condition changes. Be flexible and know your options if a change in treatment becomes necessary. Following are some goals to consider:
- Eliminating the HCC by curing it; also referred to as a curative treatment
- Shrinking the tumor(s) to make liver resection or transplantation possible; also referred to as downsizing the tumor
- Slowing the cancer’s progression to extend life
- Using supportive (palliative) care to improve your quality of life by managing side effects, treating post-operative pain and symptoms, or helping relieve pain and discomfort without active treatment
Common Ways to Treat HCC
Following are some treatment options that may be available.
Monitoring (watchful waiting) may be used if a tumor appears to be slow-growing. With close monitoring and regularly scheduled blood and imaging tests, you may be able to avoid potential side effects until treatment becomes necessary. Stay on schedule with your appointments, because your doctors may recommend treatment if the pace of the cancer increases.
Clinical trials find new and better ways to treat and potentially cure HCC. Through these research studies, advances have recently been made for treating advanced HCC. Ask your doctor if a clinical trial should be part of your care plan now or at any time during your treatment. (see Clinical Trials).
Surgery, the primary curative method for treating HCC, is often complex and requires a high degree of training and skill. You are encouraged to have treatment at a cancer facility known for performing a high volume of liver surgical procedures, and one that has liver transplant as an option. Seeking a second or third surgical opinion is recommended.
Liver resection, also called a partial hepatectomy (HEH-puh-TEK-toh-mee), may be an option if you and your liver are healthy enough to undergo an operation; your liver is functioning well; the tumors are of appropriate size and location; the disease is early-stage; and blood vessels are not invaded by the cancer. In this surgery, a wedge, entire lobe or more of the liver that contains the tumor(s), along with a margin of healthy tissue, is removed. The remaining healthy part of the liver will continue to function as it regenerates (regrows), often to near normal size.
For complex operations, a liver resection may be performed as a traditional open resection. The surgeon makes an incision into the abdomen. This is major surgery and requires significant recovery time.
Minimally invasive laparoscopic surgery may be an option for resections, depending on the tumor location and surgeon's experience. A few small incisions are made in the abdomen to insert a long, tube-like medical instrument (laparoscope) with a tiny video camera on the end. Magnified images from inside the body are transmitted to a video screen in the operating room to guide the surgeon. Although one larger incision is typically made to remove the tumor from your abdomen, this method usually results in shorter recovery time and fewer complications than traditional open resection.
Liver transplantation is a highly effective, potentially curative treatment for HCC; however, only a very small percentage of people qualify for it. Candidates must meet strict criteria concerning the size, stage, location and number of tumors present. Other factors considered include a qualifying “liver score” based on blood levels of creatinine, bilirubin, sodium and blood clotting factors. It is beneficial to have your evaluation in a center that performs liver transplants to ensure that the latest criteria for eligibility for transplant are integrated into your treatment considerations. The national and regional policies for these criteria are modified and updated relatively frequently. If your doctors believe you may be a candidate, you can be referred for assessment to a transplant team.
If you are a candidate, you will likely undergo bridging treatment while you wait for a liver to become available. Bridging therapy is designed to prevent the cancer from growing or spreading during the wait, which can sometimes be significant. Bridging treatments may include ablation, embolization, radiation therapy or systemic drug therapy.
During transplantation, the entire liver is removed (hepatectomy) and replaced with a healthy liver, most often from a deceased donor. In some cases, a living donor may be used.
Ablation destroys tumors with heat instead of removing them. It may be an option for small tumors and when surgery is not a good option. It is a better bridge to transplant than surgical resection.
Radiofrequency ablation (RFA) and microwave ablation (MWA) both involve use of imaging (typically CT scan) to guide a needle into the tumor. RFA uses radiofrequency electric current to generate heat, whereas MWA relies on electromagnetic microwaves at the tip of the probe to destroy the tumor. Both are equally effective, though MWA is used much more commonly now than RFA.
Cryoablation, also called cryosurgery or cryotherapy, is another form of ablation, but is used far less commonly than MWA and RFA. This technique involves delivery of an extremely cold gas through a hollow needle. This may also be referred to as thermal ablation.
Embolization therapies are generally not curative but can be very effective in extending life and improving quality of life.
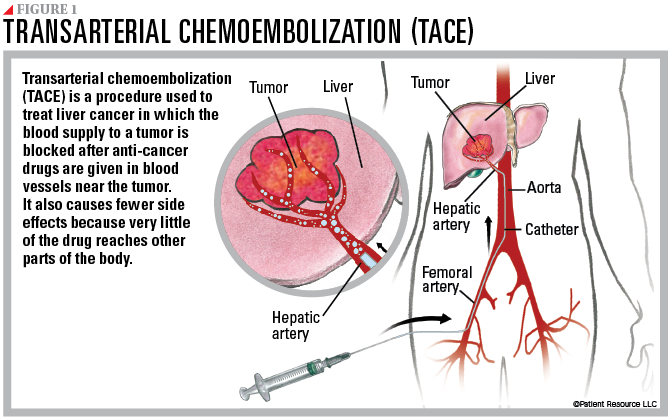
Transarterial chemoembolization (TACE) involves combines chemotherapy with embolization (see Figure 1). This minimally invasive procedure involves making a small incision in the groin and inserting a catheter, a thin, flexible tube that is guided with the help of imaging through the body to the artery that supplies blood to the liver (hepatic artery). Chemotherapy is administered into small hepatic arteries that are the main source of blood for most tumors developing in the liver. The arteries are blocked to allow the chemotherapy to remain in the area of the tumor for longer periods of time. Very little of the chemotherapy escapes the liver, making conventional side effects from chemotherapy uncommon.
Transarterial bland embolization (TAE) is similar to TACE, but chemotherapy is not used. When the catheter is in place, tiny particles made of gelatin beads or sponges are injected to block small arteries, cutting off the flow of blood feeding the tumor. Healthy liver tissue continues to receive blood from other blood vessels.
Radioembolization, also referred to as Y90 or Yttrium 90, combines radiation therapy with embolization. Microscopic glass beads containing high-dose radiation are injected into the hepatic artery to be delivered directly to the tumor. The goal is to slow the growth of the tumors and reduce symptoms, although radioembolization has also been used to reduce the size of tumors to make surgery possible.
Drug therapy may be used to manage HCC.
Targeted therapy is designed to slow the cancer’s progression by traveling through the bloodstream looking for specific proteins and tissue environments to block cancer cell signals. This, thereby, restricts the growth and spread of cancer.
An angiogenesis inhibitor is the type of targeted therapy most commonly used for HCC. Vascular endothelial growth factors (VEGFs) are commonly used.
Many targeted therapies are taken orally at home. They are systemic, which means the drugs travel throughout the body (see Figure 2). They may be used alone or in combination with immunotherapy.
Immunotherapy fights cancer by stimulating the body’s immune system to recognize and destroy cancer cells. Immune checkpoint inhibitors are the type of immunotherapy currently approved for HCC. They may be used for advanced HCC in certain instances.
These drugs prevent the immune system from slowing down, allowing it to keep up its fight against the cancer. The following checkpoint receptors are targets for immunotherapy for HCC:
- PD-1 (programmed cell death protein 1) is a receptor involved with signaling T-cells to die and reducing the death of regulatory T-cells (suppressor T-cells). PD-1 can signal the immune system to slow down only if it connects with PD-L1.
- PD-L1 (programmed death-ligand 1) is a protein that, when combined with PD-1, sends a signal to reduce the production of T-cells and enable more T-cells to die. When PD-1 (the receptor) and PD-L1 (the protein) combine, the reaction signals that it is time to slow down.
Depending on the specific treatment, immunotherapy is given intravenously (IV) or by subcutaneous injection. It may be used alone or combined with another therapy.
Radiation therapy involves high-energy X-rays or other types of radiation to destroy cancer cells. The goal is to shrink tumors or slow their growth. It may be used to relieve pain and other cancer symptoms. Your doctor may talk with you about stereotactic body radiotherapy, image-guided radiation therapy and proton beam radiation therapy.
